مرحبا بك في هذا المنتدى !
يبدو أنك جديد هنا. إذا كنت تريد أن تتورط، انقر فوق أحد هذه الأزرار!
روابط سريعة
الأقسام
- 9.5K جميع الأقسام
- العلوم الطبية الأساسية Basic Medical Sciences
- علم التشريح العام و الجنين Anatomy and Embryology
- علم وظائف الأعضاء (الفيزيولوجيا) Physiology
- علم النسج Histology
- علم النسج العام ( عدا الأسنان ) General Histology
- علم النسج الخاص بالأسنان Oral histology
- علم الخليةو الحياة Biology
- علم التشريح المرضي Pathology
- التشريح المرضي العام ( عدا الأسنان ) Pathology
- التشريح المرضي الخاص بالأسنان Oral Pathology
- علم الأحياء الدقيقة Microbiology
- الجراثيم و الفيروسات Germs and Viruses
- الطفيليات الطبية Parasitology
- الفطور و الحشرات Insects and Fungi
- علم الوراثة الطبية Medical Genetics
- علم المناعة الطبية Medical Immunology
- 4 العلوم الطبية السريرية Clinical Medical Sciences
- الأمراض الداخلية Internal Medicine
- 4 الجراحة Surgery
- التوليد و الأمراض النسائية Gynacology & Obstetrics
- الصحة الجنسية Sexual Health
- طب الأطفال Pediatrics
- الجلدية Dermatology
- العينية Ophthalamology
- انف و أذن و حنجرة Ear, Nose, and Throat
- الطب المخبري labratory Medicine
- علم الأورام Oncology
- الطب الشرعي Forensic Medicine
- الطب النفسي Psychiatric
- التغذية والطب البديل Nourishments and Alternative Medicine
- طب الطوارئ و الإسعافات الأولية Emergency Medicine And Primary aids
- متلازمات طبية Medical Syndromes
- علم الأشعة Radiology
- طب الأسنان Dental Medicine
- التعويضات المتحركة الكاملة و الجزئية Removable Prothodontics
- المداواة الترميمية operative dentistry
- المداواة اللبية Endodontics
- طب أسنان الأطفال Pediatric Dental
- جراحة الوجه والفكينoral surgery
- التعويضات الثابتة Fixed Prothodontics
- المواد السنية dental materials
- النسج حول السنية periodontology
- التقويم Orthodontics
- منتدى فنيي الأسنان dental technicians
- طب الفم العام general oral medicine
- علم الأشعة Radiology
- حالات سريريةClinical Cases
- أخر مستجدات طب الأسنان last news
- المنتدى الطبي السني العامgeneral dentistry
- علم الصيدلة Pharma
- علم الأدوية
- علم الأدوية Pharmacology
- أدوية الطوارئ Emergency drugs
- المضادات الحيوية Antibiotics
- الأدوبة المسببة للتشوهات الجنينية Teratogenic drugs
- أدوية Drugs
- علم الكيمياء Chemistry
- كيمياء حيوية سريرية Clinical Biochemistry
- الكيمياء العامة و العضوية و الفيزيائية General & organic chemistry & physical
- الكيمياء الحيوية Biochemistry
- الكيمياء التحليلية و التحليل الآلي Analytical chemistry and the automated analysis
- علم عقاقير Pharmacognosy
- الطب البديل Alternative Medicine
- علم الأعشاب الصيدلانية Pharmaceutical Herbs
- التكنولوجيا الصيدلية Pharmatical technology
- الصيدلانيات Pharmaceutics
- الصيدلة الحيوية والحرائك الدوائية Biopharmaceutics & Pharmacokinetics
- الصناعة الدوائية Drug Industry
- علم السموم Toxicology
- الوصفات الطبية Prescriptions
- صيدلية المجتمع و أدوية OTC Medicines OTC
- الكيمياء الصيدلية Pharmaceutical chemistry
- الصيدلة سريرية و صيدلية المشافي Clinical & Hospital Pharmacy
- دمويات و مناعيات hematology & immunology
- مراقبة جودة الأدوية Drug Quality Control
- البيولوجيا الجزيئية Molecular Biology
- الصحة العامة و تلوث البيئة General Health
- المنتدى الصيدلاني العام
- الجودة الغذائية Food quality
- قسم الجودة الطبية Department of Medical Quality
- قسم الجودة العام General Quality Department
- قسم السلامة والصحة المهنية Department of Occupational Safety and Health
- قسم جودة وسلامة الأغذية Department of Food Quality and Safety
- المنتدى الطبي العام
- المنتدى الطبي العام
- منتدى العلوم والتكنولوجيا الطبية Medical Technology
- قانون و أخلاقيات المهنة
- تاريخ و آداب الطب
- الدراسات العليا و الدراسة في الخارج
- امتحانات Medical Exams
- تبادل الكتب الطبية و الميديا و البيانات الطبية
- مواضيع طبية غير مصنفة
- قسم الأسرة و المجتمع
- العناية بالمرأة الحامل و المرضع
- تربية الأطفال
- الصحة العامة
- التغذية الصحية و الغذاء الصحي
- أسريات
- 2 استراحة العيادة السورية
- المنتدى العام
- نشاطات و ترفيه
- 1 إسلاميات
- تطوير الذات و البرمجة اللغوية العصبية NLP
- المنتدى التقني
- مكتبة الصور و التصميم
- 1 المنتدى الثقافي و الأدبي
- المنتدى الرياضي
- منتدى اللغات Foriegn Languages
- الساحة العامة
- ساحة الحوار و النقاش
- ترحيب و تعارف
- قسم الاستشارات الطبية
- البحوث والندوات العلمية
- الاقتراحات و التطويرات
- الأقــســـام الــعـــامــة
- منتدى الحوار العام
- المواضيع العامة القديمة المستردة
- المواضيع الحاوية على مرفقات
clinical Reports
 محمد حلبية
عضو ماسي
محمد حلبية
عضو ماسي
Management of extruded maxillary molars to accommodate a mandibular
restoration: A clinical report
restoration: A clinical report
Youn-Sic Chun, DDS, MSD, PhD,a Joon Row, DDS, MSD, PhD,b Sung-Jae Yang, DDS,c Hyun-Suk Cha,
DDS,c and Jung-Suk Han, DDS, MS, PhDd
DDS,c and Jung-Suk Han, DDS, MS, PhDd
College of Medicine, Ewha Womans University, Seoul, Korea
Prosthodontic treatment for posterior mandibular
edentulous area with the extruded opposing maxillary
segment has been a challenge to clinicians. It is necessary
to regain original space and to correct the occlusal
plane for the ideal prosthodontic treatment. Several
approaches have been introduced to solve this problem
based on the severity of supereruption: (1) no treatment;
(2) restoration of the mandibular occlusion in an
abnormal occlusal plane with a shortened prosthesis;
(3) reduction of coronal parts of the teeth to provide
restorative space and to correct the occlusal plane, it
may require endodontic treatment, periodontal surgery,
and a fixed prosthesis1; (4) surgical impaction by the
subapical osteotomy2,3; or (5) orthodontic intrusion of
the extruded teeth.4,5 Each method has advantages and
disadvantages. Consequently, the dentist will select the
treatment option according to clinical situation.
This clinical report describes the effect of combining
treatments for a patient with an extruded maxillary
segment. The posterior mandibular edentulous area
was restored with a fixed implant-supported prosthesis
after the correction of the occlusal plane, vertical
space, and contact points by using a fixed orthodontic
appliance (molar intrusion arch).
edentulous area with the extruded opposing maxillary
segment has been a challenge to clinicians. It is necessary
to regain original space and to correct the occlusal
plane for the ideal prosthodontic treatment. Several
approaches have been introduced to solve this problem
based on the severity of supereruption: (1) no treatment;
(2) restoration of the mandibular occlusion in an
abnormal occlusal plane with a shortened prosthesis;
(3) reduction of coronal parts of the teeth to provide
restorative space and to correct the occlusal plane, it
may require endodontic treatment, periodontal surgery,
and a fixed prosthesis1; (4) surgical impaction by the
subapical osteotomy2,3; or (5) orthodontic intrusion of
the extruded teeth.4,5 Each method has advantages and
disadvantages. Consequently, the dentist will select the
treatment option according to clinical situation.
This clinical report describes the effect of combining
treatments for a patient with an extruded maxillary
segment. The posterior mandibular edentulous area
was restored with a fixed implant-supported prosthesis
after the correction of the occlusal plane, vertical
space, and contact points by using a fixed orthodontic
appliance (molar intrusion arch).
CLINICAL REPORT
A 42-year-old man was evaluated for prosthodontic
treatment of the missing posterior mandibular teeth.
Clinical examination and mounted diagnostic cast
showed normal occlusal relationship from second premolar
to second premolar; however, early extraction of
the mandibular left first and second molar and right
first molar resulted in severe occlusal problems.
The mandibular right second molar was tipped
mesially and lingually, with an angular bony defect at
the mesial root. The maxillary left first and second
molar were extruded down to the edentulous mandibular
residual ridge (Fig. 1). The maximum interarch
space was 4.5 mm, so it was impossible to fabricate a
conventional implant prosthesis6 without the reduction
of a significant amount of the natural opposing dentition
treatment of the missing posterior mandibular teeth.
Clinical examination and mounted diagnostic cast
showed normal occlusal relationship from second premolar
to second premolar; however, early extraction of
the mandibular left first and second molar and right
first molar resulted in severe occlusal problems.
The mandibular right second molar was tipped
mesially and lingually, with an angular bony defect at
the mesial root. The maxillary left first and second
molar were extruded down to the edentulous mandibular
residual ridge (Fig. 1). The maximum interarch
space was 4.5 mm, so it was impossible to fabricate a
conventional implant prosthesis6 without the reduction
of a significant amount of the natural opposing dentition
or the mandibular crestal bone. After an evaluation
of mounted diagnostic casts and radiographic images,
the orthodontic molar intrusion method was chosen for
this patient to regain enough vertical space for the
implant-supported fixed prosthesis and to correct the
occlusal plane and contact point problem.
Before the orthodontic treatment, two 13-mm
Screw-Vent implants (Dentsply, Encino, Calif.) were
placed in the mandibular left posterior edentulous area
(Fig. 1). During implant surgery, periodontal treatment
of the mandibular left second premolar was performed.
The Molar Intrusion Arch was constructed
of mounted diagnostic casts and radiographic images,
the orthodontic molar intrusion method was chosen for
this patient to regain enough vertical space for the
implant-supported fixed prosthesis and to correct the
occlusal plane and contact point problem.
Before the orthodontic treatment, two 13-mm
Screw-Vent implants (Dentsply, Encino, Calif.) were
placed in the mandibular left posterior edentulous area
(Fig. 1). During implant surgery, periodontal treatment
of the mandibular left second premolar was performed.
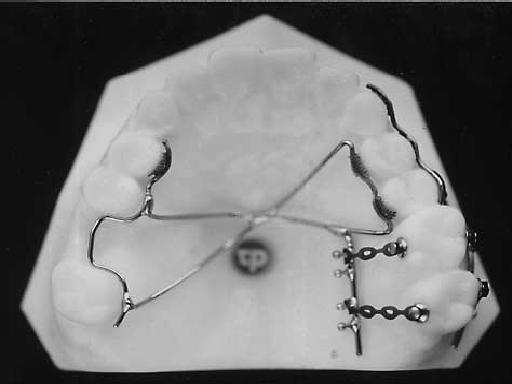
The Molar Intrusion Arch was constructed
to intrude the maxillary left first and second molar
(Fig. 2). Buttons were bonded on both buccal and
palatal sides of the maxillary molars for power chains
to apply orthodontic force through the center of resistance
of the each maxillary molar. Intrusion force was
50g per side (Fig. 2).
Molar intrusion arch is a simple fixed bonded appliance.
To level extruded posterior segment into the
correct position, 3 points should be considered for the
orthodontic treatment:
1. Anchorage. The appliance should be rigid and
include as many teeth as possible. The Molar Intrusion
Arch was made with 0.9 mm stainless steel wire and
the crossing area should be soldered.
2. Force application point. To apply intrusive force
through the center of resistance of molars, the buccopalatal
approach was used.
3. Amount of force. To intrude a single rooted
tooth, 15 to 20g of force is usually recommended7;
therefore, 50 to 60g of force was assumed to be
required to intrude a maxillary molar with 3 roots
(Fig. 2). Buttons were bonded on both buccal and
palatal sides of the maxillary molars for power chains
to apply orthodontic force through the center of resistance
of the each maxillary molar. Intrusion force was
50g per side (Fig. 2).
Molar intrusion arch is a simple fixed bonded appliance.
To level extruded posterior segment into the
correct position, 3 points should be considered for the
orthodontic treatment:
1. Anchorage. The appliance should be rigid and
include as many teeth as possible. The Molar Intrusion
Arch was made with 0.9 mm stainless steel wire and
the crossing area should be soldered.
2. Force application point. To apply intrusive force
through the center of resistance of molars, the buccopalatal
approach was used.
3. Amount of force. To intrude a single rooted
tooth, 15 to 20g of force is usually recommended7;
therefore, 50 to 60g of force was assumed to be
required to intrude a maxillary molar with 3 roots
If the orthodontic force is excessive, anchorage loss
will occur instead of intrusion of maxillary molars and
cause extrusion of the anchorage teeth. In addition, a
0.017 × 0.025 TMA wire spring was used to upright
the mandibular right second molar and restore with a
conventional fixed partial denture (FPD). During the
uprighting procedure, occlusal adjustment was performed
to eliminate premature contacts.
After 3 months of healing, implants were uncovered
and abutments were connected. A provisional
acrylic resin prosthesis was constructed for implants
and has been functioning for 3 months until the
completion of orthodontic treatment. Six months
after initial orthodontic treatment, intrusion of the
maxillary left first and second molar and uprighting
of the mandibular right second molar were obtained
(Fig. 3). Conventional FPDs were fabricated to
restore other parts of the mouth. Finally, a ceramometal
fixed implant prosthesis was delivered to
the patient (Fig. 4). Posttreatment cephalometric
analysis showed a 3-mm intrusion and no pocket
will occur instead of intrusion of maxillary molars and
cause extrusion of the anchorage teeth. In addition, a
0.017 × 0.025 TMA wire spring was used to upright
the mandibular right second molar and restore with a
conventional fixed partial denture (FPD). During the
uprighting procedure, occlusal adjustment was performed
to eliminate premature contacts.
After 3 months of healing, implants were uncovered
and abutments were connected. A provisional
acrylic resin prosthesis was constructed for implants
and has been functioning for 3 months until the
completion of orthodontic treatment. Six months
after initial orthodontic treatment, intrusion of the
maxillary left first and second molar and uprighting
of the mandibular right second molar were obtained
(Fig. 3). Conventional FPDs were fabricated to
restore other parts of the mouth. Finally, a ceramometal
fixed implant prosthesis was delivered to
the patient (Fig. 4). Posttreatment cephalometric
analysis showed a 3-mm intrusion and no pocket
space for osteotomy, and sometimes it cannot correct
the axis and contact point problems.
Even though orthodontic treatment takes more
time when compared with other treatment options, it
has many advantages. For example, it is more conservative;
one can avoid surgical risk; costs are lower; and
prosthodontic treatment is simpler. In addition to
these advantages, it provides proper dento-alveolar
relationship such as long-axis control, buccolingual
position, and contact points without any harm to teeth
and supporting alveolar bone.
For periodontal considerations, professional oral
prophylaxis and plaque control are needed throughout
the treatment period to avoid any adverse periodontal
reactions. With the use of the Molar Intrusion Arch in
a controlled manner, orthodontic force can be applied
to both buccal and palatal side through the center of
resistance of the extruded molar more accurately.
This clinical report demonstrates that orthodontic
treatment can improve the environment of difficult situations
for prosthodontic treatment and provide a
favorable long-term prognosis.
the axis and contact point problems.
Even though orthodontic treatment takes more
time when compared with other treatment options, it
has many advantages. For example, it is more conservative;
one can avoid surgical risk; costs are lower; and
prosthodontic treatment is simpler. In addition to
these advantages, it provides proper dento-alveolar
relationship such as long-axis control, buccolingual
position, and contact points without any harm to teeth
and supporting alveolar bone.
For periodontal considerations, professional oral
prophylaxis and plaque control are needed throughout
the treatment period to avoid any adverse periodontal
reactions. With the use of the Molar Intrusion Arch in
a controlled manner, orthodontic force can be applied
to both buccal and palatal side through the center of
resistance of the extruded molar more accurately.
This clinical report demonstrates that orthodontic
treatment can improve the environment of difficult situations
for prosthodontic treatment and provide a
favorable long-term prognosis.
depth of more than 2 mm could be detected around
the intruded teeth.
the intruded teeth.
DISCUSSION
Among the treatment options for extrusion opposing
dentition, the orthodontic molar intrusion was the
best choice for this patient to correct the interocclusal
space and plane of occlusion, for restoration of the left
posterior edentulous mandible with a fixed implant
prosthesis. For example, the reduction of opposing
extruded maxillary molars required endodontic treatment
and additional crowns. The surgical impaction of
extruded teeth requires sufficient mesial and distal
dentition, the orthodontic molar intrusion was the
best choice for this patient to correct the interocclusal
space and plane of occlusion, for restoration of the left
posterior edentulous mandible with a fixed implant
prosthesis. For example, the reduction of opposing
extruded maxillary molars required endodontic treatment
and additional crowns. The surgical impaction of
extruded teeth requires sufficient mesial and distal
REFERENCES
1. Zarb GA, Bergman B, Clayton JA, Mackay HF. Prosthodontic treatment
for partially edentulous patients. St Louis: CV Mosby; 1978. p. 21-4, 42.
2. Kaminish RM. Segmental osteotomies to optimize restorative procedures.
Oral Maxillofac Surg 1989;1:1-28.
3. Alexander JM, Van Sickels JE. Posterior maxillary osteotomies: an aid for
a difficult prosthodontics problem. J Prosthet Dent 1979;41:614-7.
4. Melsen B, Fiorelli G. Upper molar intrusion. J Clin Orthod 1996;30:91-
6.
5. Bonetti GA, Giunta D. Molar intrusion with a removable appliance. J
Clin Orthod 1996;30:434-7.
6. Engelman MJ. Clinical decision making and treatment planning in
osseointegration. Chicago: Quintessence Publishing Co, Inc; 1996. p.
104.
7. Proffit WR. Contemporary orthodontics. St Louis: Mosby, Inc; 1993. p.
for partially edentulous patients. St Louis: CV Mosby; 1978. p. 21-4, 42.
2. Kaminish RM. Segmental osteotomies to optimize restorative procedures.
Oral Maxillofac Surg 1989;1:1-28.
3. Alexander JM, Van Sickels JE. Posterior maxillary osteotomies: an aid for
a difficult prosthodontics problem. J Prosthet Dent 1979;41:614-7.
4. Melsen B, Fiorelli G. Upper molar intrusion. J Clin Orthod 1996;30:91-
6.
5. Bonetti GA, Giunta D. Molar intrusion with a removable appliance. J
Clin Orthod 1996;30:434-7.
6. Engelman MJ. Clinical decision making and treatment planning in
osseointegration. Chicago: Quintessence Publishing Co, Inc; 1996. p.
104.
7. Proffit WR. Contemporary orthodontics. St Louis: Mosby, Inc; 1993. p.


Fig 1. Before treatment. A, Intraoral view; B, panoramic
radiograph. Maxillary left molars showed supereruption
and marginal ridge step. Two implants were placed in
mandibular left posterior edentulous area

radiograph. Maxillary left molars showed supereruption
and marginal ridge step. Two implants were placed in
mandibular left posterior edentulous area
Fig. 2. Molar intrusion arch. A, Model view; B, intraoral
view


view
Fig. 3. Periapical views. A, Pretreatment; B, posttreatment.
Correction of bone level, marginal ridge, and contact point
relation


Correction of bone level, marginal ridge, and contact point
relation
Fig. 4. Final fixed implant prosthesis. A, Intraoral view; B,
panoramic radiograph. Correction of occlusal plane, contact
points, and increased vertical space for fixed implant
prosthesis
.
panoramic radiograph. Correction of occlusal plane, contact
points, and increased vertical space for fixed implant
prosthesis
.
التعليقات
دائما متميز في مواضيعك
مشكور دكتور عمار