Radiotherapy marks علامات المعالجة الشعاعية
HTML clipboard
INSTRUCTION
Look at this patient's chest.
PATIENT 1
Salient features
History
-
History of breast cancer.
-
Ask about chemotherapy and schedule of radiotherapy.
Examination
-
Telangiectasia over the chest wall.
-
There may be a unilateral mastectomy.
Diagnosis
This patient has telangiectasia and a unilateral mastectomy (lesion), indicating that shehas had radiotherapy (aetiology) for breast cancer in the past.
PATIENT 2
· India ink marks over the chest .
* Localized erythema in the same region.
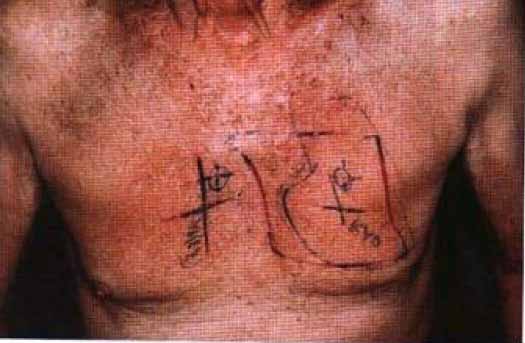
Diagnosis
This patient has India ink marks over the chest with localized erythema (lesion) indicating that she is currently undergoing radiotherapy treatment (aetiology).
ADVANCED-LEVEL QUESTIONS
Which other normal tissues, apart from the skin, are affected by radiation therapy?
Tissues that exhibit early or late damage from radiation therapy include mucosa, spinal cord, bone marrow and lymphoid system. To minimize these effects, radiation is normally delivered in a tYactionated manner to allow recovery of normal host tissues (but not of tumour ).
What modalities may be used to minimize the side-effects of radiation?
-
Fractionation of dose.
-
Rendering the tumour more sensitive to radiotherapy by prior chemotherapy and thereby reducing the dose.
-
Regional hyperthermia (40-42°C), particularly in superficial tumours and relatively bulky non-vascular tumours.
-
Radiolabelled antibodies which deliver high levels of radiation locally to the tumour bed.
How is radiotherapy usually delivered ?
It is usually delivered either as brachytherapy (where the radiation source is close to the tumour) or as teletherapy (where supervoltage radiotherapy is usually delivered with alinear accelerator).
In which conditions is radiotherapy beneficial ?
Malignant conditions
-
Radiotherapy as the sole agent with a curative intent: in Hodgkin's disease ,some neoplasms of brain and spinal cord, oral cavity, pharynx, oesophagus , laryngeal tumours permitting cure without loss of voice, tumours of cervix and vaginal cavity.
-
Radiation with surgery: in cancers of lung, breast, urinary bladder, seminomas,ovary, uterus, sarcomas of soft tissue and testicular seminomas .
-
Radiation as adjuvant to chemotherapy: lymphomas, lung cancers and childhood cancers.
-
Radiation as palliative therapy for pain and/or dysfunction: superior vena cava obstruction, dysphagia of terminal illness, upper airway obstruction, spinal cord compression, pericardial tamponade secondary to malignant pericardial tumours.
Non-malignant conditions
-
Exophthalmos.
-
Rheumatoid arthritis (total lymphoid irradiation is an experimental therapeutic procedure).
-
Ankylosing spondylitis, where local external irradiation of an involved peripheral joint or injected radiation synovectomy can be valuable in ameliorating pain and allowing mobility.
-
Spinal irradiation is no longer used because of the risk of haematological malignancy.
-
Intracoronary radiation can significantly reduce restenosis rates after angioplasty (Circulation 2000; 101: 360-5).
What are the side-effects of radiotherapy ?
-
Acute toxicity: systemic symptoms including malaise, fatigue, anorexia, nausea and vomiting; diarrhea and local skin and mucosal changes. Bone marrow suppression may occur following irradiation to the pelvis and long bones.
-
Long-term toxicity: cutaneous hyperpigmentation, impaired function of irradiated viscera, bone necrosis, myelopathy and secondary malignancies.
The use of irradiation began shortly after the discovery of X-rays by Roentgen in 1895(Lancet 1997; 349 (suppl II): 1-3).Allen Lichter is radiation oncologist and Dean of the University of Michigan School of Medicine (Lichter AS, Lawrence TS 1995 Recent advances in radiation oncology. NEngl J Med 332: 371-7). He was recently nominated by the Institute of Medicine ,National Academy of Sciences, USA, for his contributions which include three-dimensional treatment planning and conformal radiotherapy of cancers.