Rosacea العد الوردي (حب الشباب)
HTML clipboard
INSTRUCTION
Look at this patient.
SALIENT FEATURES
History
-
Intermittent facial flushing.
-
Blushing of the face by caffeine, alcohol or spicy foods.
-
History of unilateral headaches (an increased incidence of migrainousheadaches accompanying rosacea has been reported).
Examination
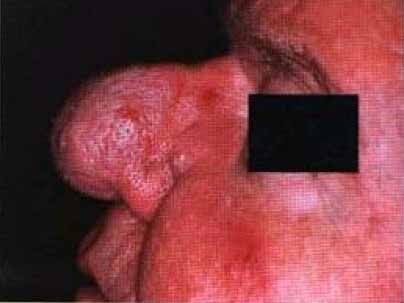
Red patch with telangiectasia, acneiform papules, and pustules overlying the flushareas of the face, i.e. cheeks, chin and nose. (The papules and pustulesdistinguish it from the rash of SLE.)

Proceed as follows:
-
Comment on the following:
-
-Rhinophyma ( irregular thickening of the skin of the nose with enlargedfollicular orifices).
-
- Blepharitis, conjunctivitis.
-
Tell the examiner that you would like to obtain an ophthalmological evaluationfor chalazion and progressive keratitis which can lead to scarring and blindness.
DIAGNOSIS
This patient has a red patch on the face with papules and pustules (lesion) due torosacea (aetiology) which is cosmetically disfiguring (functionalstatus).
ADVANCED-LEVEL QUESTIONS
How would you distinguish rosacea from acne?
Rosacea is distinguished from acne by age (middle-aged and older people), thepresence of a vascular component (i.e. rosy hue, erythema and telangiectasia) and theabsence of comedones.
How would you manage such a patient?
-
Avoid factors that provoke facial flushing.
-
Tetracycline or metronidazole.
-
Hydrocortisone cream.
-
Retinoids - in resistant disease.
-
Yellow light laser for telangiectasia.
-
Surgical removal for rhinophyma.
What are the causes of red face in an adult?
Malar rash of SLE, heliotrope rash of dermatomyositis, seborrhoeic dermatitis andperioral dermatitis.